Welcome to Part One of our series on the Benefits of Babywearing. Watch this space, or come along to one of our free Babywearing Workshops to find out more.
Details of our next Babywearing Workshop can be found on our events page.
Baby-wearing can be immensely enjoyable and mutually beneficial for all involved. Among the many benefits of babywearing, the Chiropractor in me loves the way babywearing can promote optimal spine and nervous system development. The busy mum in me loves the convenience baby wearing can offer, and I personally love the connection I feel with my daughter while using it, we can look in each other eyes and explore the world together, talking or babbling about all that we see, while holding each other close.
In no particular order, here are some of the many benefits of babywearing:
PROMOTING OPTIMAL SPINE DEVELOPMENT
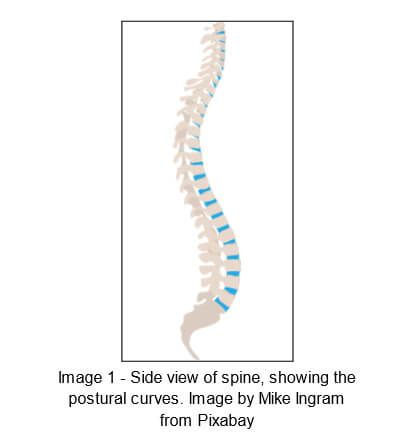
A baby’s spine is not just a smaller version of an adults spine. It is mostly made of cartilage (so softer) at birth, and normal postural curves are not fully developed. Normal postural curves give our spines the perfect balance of strength and flexibility needed to navigate upright life in a gravitational world.
In the adult spine, when viewed from the side, we have 3 C-shaped curves (see image 1 below). A forward facing curve in the neck (cervical lordosis), a backwards facing curve in the upper and mid back (thoracic kyphosis) and a forwards facing curve in the lower back (lumbar lordosis).
The benefits of these curves are that they:
- Resist the axial compressive force of gravity. Where the amount of resistance is equal to the number of curves.. So a spine with 3 fully developed postural curves has a spine strength of 10/10. The loss of just one of these curves, effectively halves the strength of the spine to 5/10
- Provide optimal muscle attachment and efficiency of movement
- Decrease stress on spine
- Produce optimal length/tension on the spinal cord
- Provide mechanical advantage for stabilising and moving an upright head and allow upright standing position

Babies are born in the “fetal” position, with one backwards C-shaped ‘kyphotic’ curve in their spine. As their neck muscles develop to hold their heads up against gravity, a forwards C-shaped ‘lordotic’ neck curve develops. Then as they start to crawl and walk, the forces of gravity and latent tightness in the muscles at the front of their bodies encourages the development of the forwards C-shaped ‘lordotic’ lumbar curve.
An appropriately selected and utilised (see TICKS guidelines below) baby-wearing product will conform to the baby’s natural spinal curve/curves, providing good support, whilst neither allowing the spine to slump into a more flexed position nor force the spine into a more extended (straightened) position.
Being slumped into a more flexed position can not only effect the spine, but can also interfere with airflow and breathing, digestion and many other normal body functions.
Utilising the UK Sling Consortium’s TICKS safety guidelines can minimise the risk of this.

TICKS Guidelines. Image from http://babyslingsafety.co.uk. Guidelines by the UK Sling Consortium
TIGHT – slings and carriers should be tight enough to hug your baby close to you as this will be most comfortable for you both. Any slack/loose fabric will allow your baby to slump down in the carrier which can hinder their breathing and pull on your back.
IN VIEW AT ALL TIMES – you should always be able to see your baby’s face by simply glancing down. The fabric of a sling or carrier should not close around them so you have to open it to check on them. In a cradle position your baby should face upwards not be turned in towards your body.
CLOSE ENOUGH TO KISS – your baby’s head should be as close to your chin as is comfortable. By tipping your head forward you should be able to kiss your baby on the head or forehead.
KEEP CHIN OFF CHEST – a baby should never be curled so their chin is forced onto their chest as this can restrict their breathing. Ensure there is always a space of at least a finger width under your baby’s chin.
SUPPORTED BACK – in an upright carry a baby should be held comfortably close to the wearer so their back is supported in its natural position and their tummy and chest are against you. If a sling is too loose they can slump which can partially close their airway. (This can be tested by placing a hand on your baby’s back and pressing gently – they should not uncurl or move closer to you.)
A baby in a cradle carry in a pouch or ring sling should be positioned carefully with their bottom in the deepest part so the sling does not fold them in half pressing their chin to their chest.
Following the TICKS guidelines not only gives the babwearer the opportunity to easily and regularly check that their baby is still in a good position, but also promotes the baby’s visual and emotional development (more about that later).
Forcing the spine into a more extended position has the potential to place undue stress on the kyphotic curve, and can interfere with normal spinal curve development, potentially reducing the strength and flexibility of the spine.
PROMOTING HEALTHY HIP DEVELOPMENT
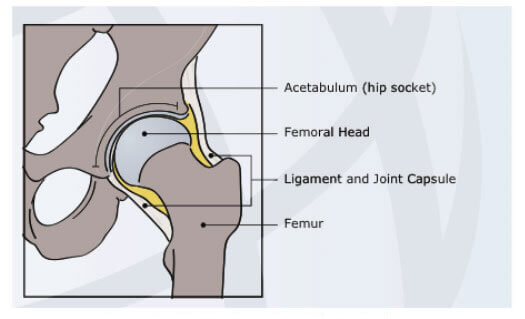
Hip Anatomy from hipdysplasia.org
The hip joint is a ball and socket type joint, with the femoral head making up the ball, and the acetabulum being the socket. Healthy hip development is dependant upon the femoral head (top of the leg), maintaining close alignment (congruent positioning) with the acetabulum (hip socket).
The femoral head is cartilaginous at birth, and is therefore more malleable than an adults.
The acetabulum is shallow and faces mores anterior and lateral (forwards and sideways) than an adults.
Angles decrease gradually with age due to modelling of the acetabulum by the femoral head and/or the maturing of the bone of the acetabular roof; as the hip changes from the intrauterine position of flexion and abduction, to the erect position of extension and adduction. Alignment is essential for the ball and socket to develop congruently.
Some common causes of misalignment include intrauterine constraint, birth trauma, breech position, tight swaddling… For more details see www.hipdysplasia.org.
If the hip dislocates at or shortly after birth, and remains undetected and uncorrected, the acetabulum doesn’t change direction and remains anterior and lateral, leading to hip dysplasia. This is why hips are checked soon after birth, and again at the 6 week check-up, as with early detection and correction, the hip can develop normally.
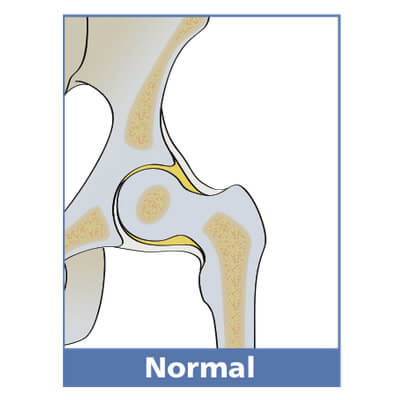
Healthy ball and socket hip alignment
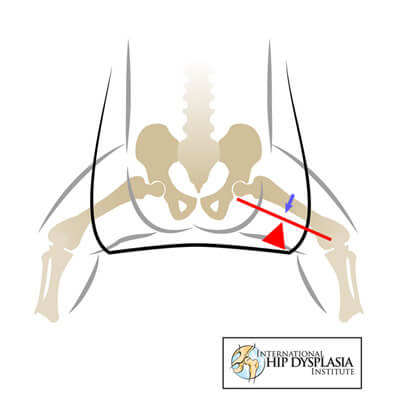
Healthy hip alignment in the squatting straddle position, with knee-to-knee support in a carrier.
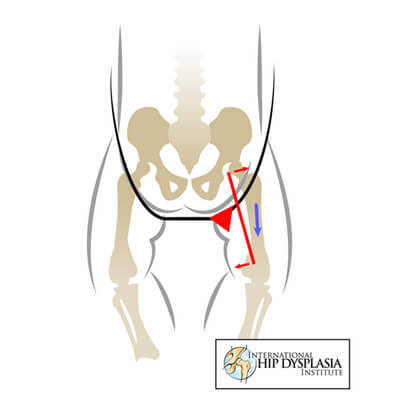
The potential impact on hip alignment when legs are extended or adducted.
The squatting straddle position (where hips are flexed (bent up) 100-110 degrees, and abducted (taken out sideways) 45 degrees), (see image 6 above) utilised when babywearing, places the ball and socket of the hip in optimal congruent positioning. This can be great for not only keeping hips healthy, but for also correcting hip issues.
To support this positioning in a baby carrier, the material supporting the bottom should also support the thighs, from knee-to-knee. (This is one of the reasons why outward facing is not recommended for young babies.)
In a sling, it is important the legs aren’t extended and/or adducted (bought together), to avoid stressing the hip. See hipdysplasia.org for more information.
Wrong

Showing less optimal/not ideal positioning
Right
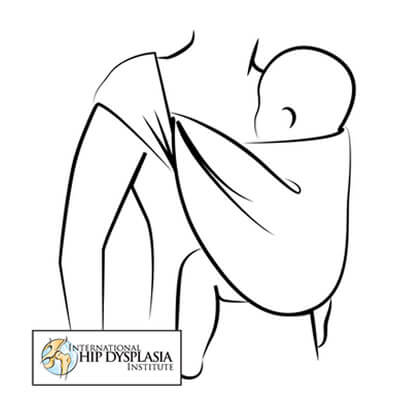
This demonstrates optimal use of sling

A carrier that hinders or impedes healthy hip development

A carrier for healthy hip development